Large Skeletal Bite Differences
Severe underbites, overbites, open bites, and crossbites can reflect jaw-position issues rather than tooth-position issues alone.

When the jaw relationship is a major part of the problem, orthodontics alone may not be enough. Surgical case orthodontics combines tooth movement with oral and maxillofacial surgery so the teeth and jaws can be corrected together in a more stable, functional way.
These cases are typically coordinated in phases. Orthodontic treatment usually happens both before and after jaw surgery to prepare the arches, support precise surgical planning, and refine the bite once the jaws are in their new position.
Surgical orthodontics is usually considered when the mismatch between the upper jaw, lower jaw, or facial proportions is too significant to predictably correct with orthodontic or expansion. The goal is not just straighter teeth. It is a healthier bite, better facial harmony, and a result that fits the anatomy more naturally in a lasting way.
Severe underbites, overbites, open bites, and crossbites can reflect jaw-position issues rather than tooth-position issues alone.
If the jaws are off center, vertically disproportionate, or retrusive, surgery may be part of creating better facial support and balance.
Difficulty chewing, unstable contacts, speech challenges, excessive incisor wear, or a bite that cannot seat well may point to a jaw-based issue.
In select adult patients, jaw advancement may be discussed when retrusive jaws and airway concerns are part of the overall diagnosis.
Orthodontics can align teeth beautifully, but it cannot fully reposition the jaws. Surgery is usually discussed when the anatomy needs skeletal correction for better function, facial support, improved balance, or long-term stability.
If the upper and lower jaws are mismatched, camouflage may straighten the teeth without truly fixing the underlying relationship.
When contacts are unstable or function is compromised, skeletal correction may create a more solid, repeatable bite.
Some cases need jaw repositioning to improve balance, symmetry, or lip and chin support in a way orthodontics alone cannot.
In some adults, jaw advancement is part of a broader discussion around airway anatomy, sleep-disordered breathing, and overall facial structure.
Not every surgical case involves both jaws. Some patients may hear upper-jaw-only or lower-jaw-only terms during planning, depending on where the skeletal correction is needed most.
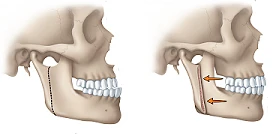
If the upper jaw is the main issue, the surgeon may discuss upper jaw surgery or maxillary surgery.
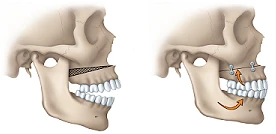
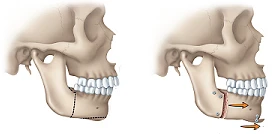
If the lower jaw is the main issue, you may hear lower jaw surgery or mandibular surgery.
Double jaw surgery means the upper jaw and lower jaw are both brought forward or repositioned together in a planned way. In carefully selected adult patients, that forward movement can improve skeletal support and create more room behind the tongue and soft palate.
Orthodontically, MMA cases still follow the same overall sequence: records and diagnosis, presurgical alignment and decompensation, surgical jaw advancement, then postsurgical bite detailing and retention.
Most surgical cases follow a coordinated sequence rather than a single event. Records and planning come first, orthodontics prepares the teeth and arches, surgery repositions the jaws, and postsurgical orthodontics finishes the details so the bite functions well long term.
Photos, digital scans, x-rays, and surgeon-orthodontist planning define the goals and sequence.
Teeth are aligned and decompensated so the jaws can be corrected accurately at surgery.
The oral surgeon repositions one jaw or both jaws based on the treatment plan and skeletal diagnosis.
Orthodontics refines the bite, coordinates contacts, and transitions into long-term retention.
This phase is where braces or aligners do the detailed setup work. Teeth are leveled, aligned, coordinated within each arch, and positioned over the supporting bone so the surgeon can move the jaws into the correct relationship.
In many surgical cases, the bite can look more pronounced during this stage because the orthodontics is removing compensation rather than disguising the discrepancy. In other words, the bite relationship may temporarily appear worse before surgery so the jaws can be corrected more accurately. That is often an expected part of building toward the surgical correction.
Presurgical orthodontics is not about making the bite look better right away. It is about setting up the teeth so the surgical move can be accurate and stable.
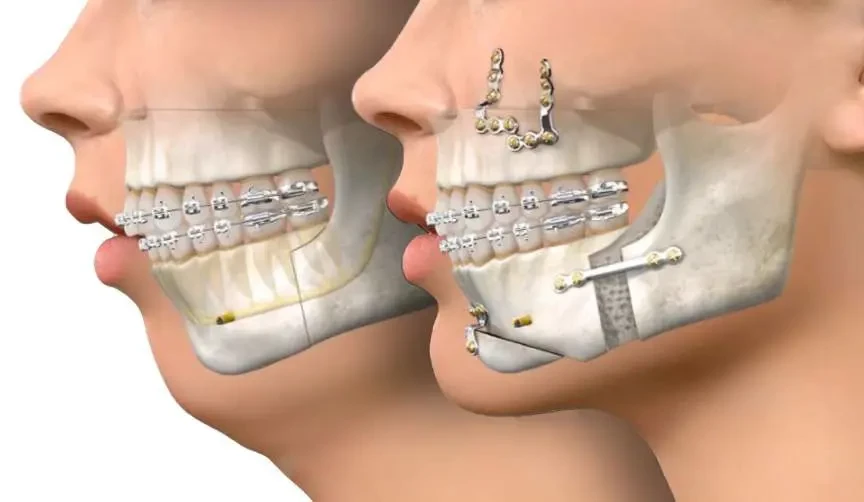
Once the teeth are prepared, the oral and maxillofacial surgeon performs the planned surgical move. Depending on the case, that may involve the upper jaw, the lower jaw, or both jaws together. Some plans also include chin surgery or other supporting procedures when indicated.
Orthodontics and surgery work as one plan here. The orthodontist prepares the tooth positions and occlusion; the surgeon repositions the jaws; and both providers use the same planning goals for function, fit, and facial balance.
Shared diagnosis between the orthodontist and oral surgeon, including whether the issue is primarily dental, skeletal, or both.
Digital planning so tooth position, jaw position, and facial goals are coordinated before the surgical date.
Postsurgical communication to guide elastics, bite settling, and final orthodontic detailing after healing begins.
After surgery, orthodontic treatment continues. This stage is usually more about finishing and settling than major tooth movement. The bite is refined, upper and lower contacts are coordinated, and any remaining detailing is completed as healing progresses.


A surgical consultation starts with diagnosis, not assumptions. We evaluate the teeth, jaws, facial structure, and bite together so we can determine whether orthodontics alone is enough or whether coordinated jaw-surgery planning would create a healthier and more stable result.